The clinical landscape of geriatric medicine is currently undergoing a significant shift as healthcare professionals move toward more proactive interventions for age-related muscle deterioration. As the concluding installment of the British Journal of Sports Medicine’s "Strong for Life" series, this report synthesizes the critical findings regarding sarcopenia—a condition characterized by the progressive and generalized loss of skeletal muscle mass and strength. While often overshadowed by more visible chronic illnesses, sarcopenia is increasingly recognized as a primary driver of frailty, loss of independence, and increased mortality in the elderly. The medical community now emphasizes that this condition is not an inevitable consequence of aging, but rather a modifiable clinical state that responds robustly to targeted physical and nutritional interventions.
Understanding the Silent Epidemic of Muscle Loss
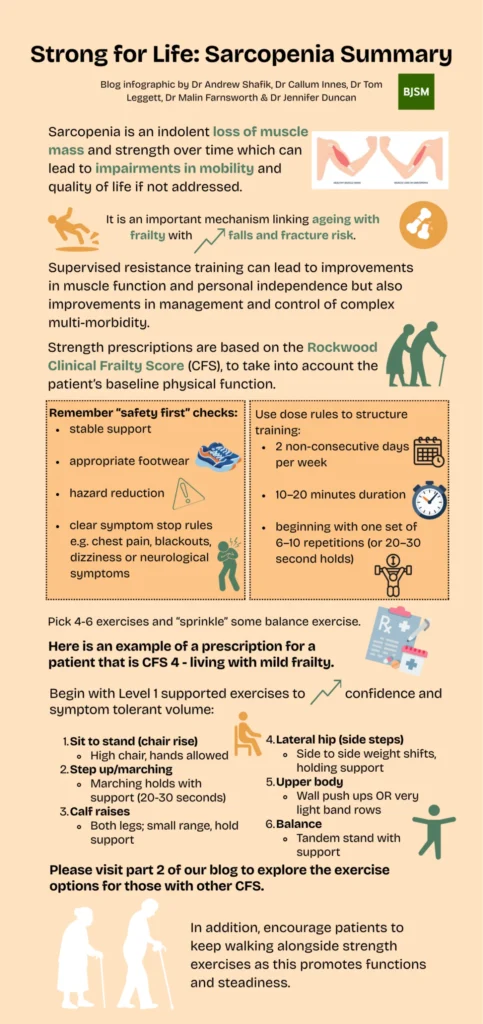
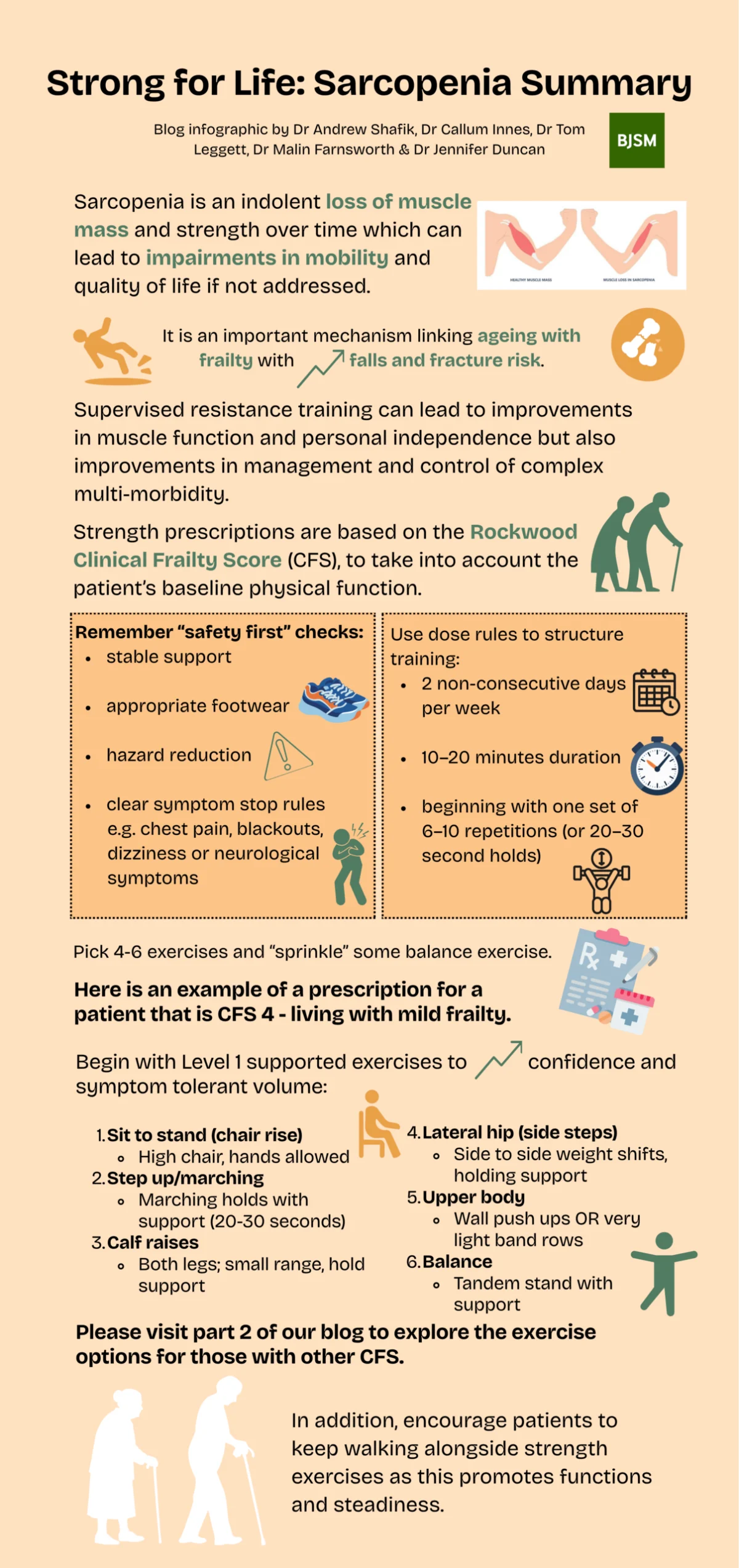
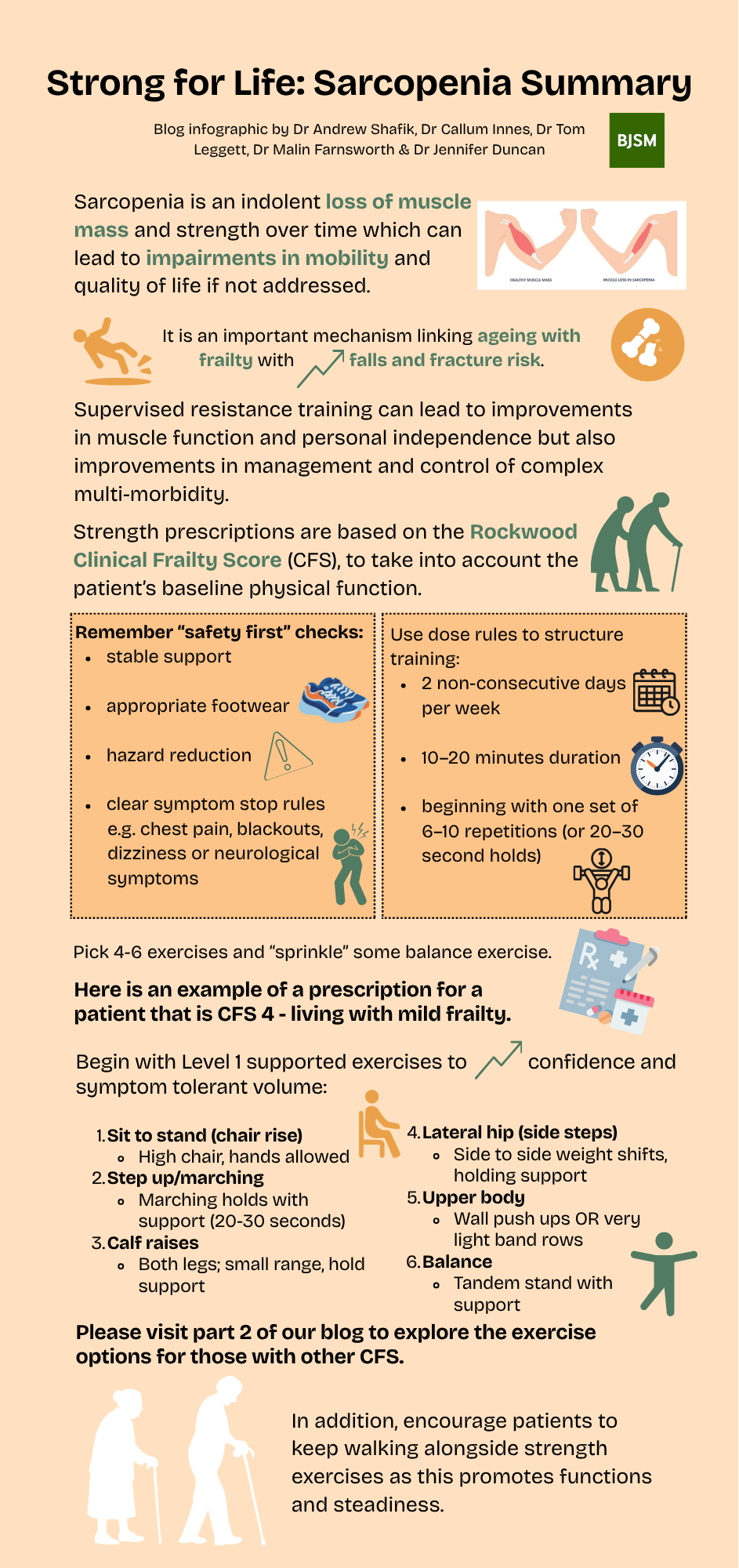
Sarcopenia remains one of the most frequently overlooked diagnoses in primary care, yet its implications for public health are profound. The condition is defined by a decline in muscle quantity and quality, which directly impairs physical performance. According to recent clinical reviews, the prevalence of sarcopenia among individuals aged 60 and older ranges from 5% to 13%, with the figure rising to as high as 50% in those over the age of 80. Despite these numbers, the "Strong for Life" series highlights that the diagnostic rate remains low, often because the gradual loss of strength is dismissed as a normal part of the aging process.
The distinction between chronological aging and pathological muscle loss is vital. While humans naturally lose approximately 1% to 2% of muscle mass annually after the age of 50, sarcopenia accelerates this process, often exacerbated by sedentary lifestyles, poor nutrition, and systemic inflammation. When left unmanaged, the condition creates a downward spiral: decreased muscle mass leads to reduced activity, which in turn leads to further muscle wasting and an increased risk of falls, fractures, and prolonged hospitalizations.
A Chronology of Clinical Recognition: From Concept to Diagnosis
The medical understanding of sarcopenia has evolved rapidly over the last four decades, moving from a vague observation of muscle loss to a strictly defined clinical diagnosis.
- 1989: Dr. Irwin Rosenberg first coined the term "sarcopenia" (derived from the Greek words for "poverty of flesh") to draw attention to the importance of muscle mass in the aging population.
- 2010: The European Working Group on Sarcopenia in Older People (EWGSOP) published the first international consensus on the definition and diagnosis of the condition, establishing it as a distinct clinical entity.
- 2016: Sarcopenia was officially granted an ICD-10-CM code (M62.84), a landmark moment that allowed for formal billing, better data collection, and increased clinical research.
- 2018-2019: The EWGSOP2 updated its guidelines, shifting the focus from muscle mass to muscle strength as the primary indicator of the condition, recognizing that strength is a better predictor of adverse outcomes than mass alone.
- 2024-Present: Current initiatives, such as the "Strong for Life" series, aim to bridge the gap between academic research and bedside practice, advocating for universal screening in geriatric care.
The Statistical Reality: Global Prevalence and Economic Burden
The economic and social costs of sarcopenia are staggering. Data from the World Health Organization (WHO) and various national health services indicate that sarcopenia significantly increases the cost of care for elderly patients. In the United States alone, the healthcare costs associated with sarcopenia were estimated at $18.5 billion annually in the early 2000s, a figure that has likely doubled when adjusted for inflation and the aging "Baby Boomer" demographic.
Individuals with sarcopenia are 2.3 times more likely to experience a fall and 3.4 times more likely to suffer a hip fracture compared to those with healthy muscle function. Furthermore, the presence of sarcopenia in patients with multi-morbidity—such as type 2 diabetes, chronic obstructive pulmonary disease (COPD), or heart failure—is linked to a 40% increase in the risk of all-cause mortality. These statistics underscore the urgency of the "Strong for Life" initiative’s call for early detection and supervised resistance training.
Diagnostic Framework: The EWGSOP2 Guidelines
The "Strong for Life" series emphasizes the use of the EWGSOP2 "Find-Assess-Confirm-Severity" (FACS) pathway. This framework allows clinicians to identify at-risk individuals before they reach a state of irreversible frailty.
- Case Finding: Utilizing the SARC-F questionnaire, a five-item self-report tool that evaluates strength, assistance with walking, rising from a chair, climbing stairs, and falls.
- Assessment: Measuring muscle strength, typically through handgrip strength or the "Chair Stand Test." For men, a grip strength of less than 27 kg is considered low; for women, the threshold is less than 16 kg.
- Confirmation: Using Dual-energy X-ray Absorptiometry (DXA) or Bioelectrical Impedance Analysis (BIA) to quantify muscle mass and quality.
- Severity Determination: Evaluating physical performance through gait speed tests or the Short Physical Performance Battery (SPPB). A gait speed of ≤0.8 m/s often indicates severe sarcopenia.
Intervention Strategies: The Role of Supervised Resistance Training
The cornerstone of the "Strong for Life" series is the advocacy for supervised resistance training (RT) as the primary treatment for sarcopenia. Unlike aerobic exercise, which improves cardiovascular health, resistance training specifically targets the neuromuscular system to induce hypertrophy and increase force production.
Medical experts involved in the series argue that resistance training acts as a "polypill" for the elderly. It stimulates the release of myokines—signaling molecules produced by muscle fibers—which have anti-inflammatory effects and improve insulin sensitivity. This makes RT particularly effective for managing complex multi-morbidity. To be effective, the training must be progressive, meaning the load or intensity must increase as the individual becomes stronger.
Supervision is emphasized as a critical factor for success. Elderly patients often harbor a fear of injury, which leads to "under-dosing" of exercise. A supervised environment ensures safety, proper technique, and the achievement of the necessary intensity to trigger muscle protein synthesis. Research shows that even individuals in their 90s can achieve significant gains in muscle power and functional independence through 12 to 24 weeks of consistent resistance training.
Nutritional Synergies: Protein and Beyond
While exercise is the primary stimulus, nutrition provides the building blocks for muscle repair. The "Strong for Life" findings suggest that the Recommended Dietary Allowance (RDA) for protein—currently 0.8 grams per kilogram of body weight—may be insufficient for the elderly. To overcome "anabolic resistance" (the reduced ability of older muscles to respond to protein intake), experts recommend a daily intake of 1.2 to 1.5 grams of protein per kilogram of body weight.
Leucine, a branched-chain amino acid, is highlighted as a key "trigger" for muscle protein synthesis. Supplementation with Vitamin D is also recommended, as Vitamin D receptors are found directly on muscle cells, and deficiency is strongly correlated with muscle weakness and an increased risk of falls.
Official Responses and Expert Perspectives
Leading voices in sports medicine and gerontology have lauded the "Strong for Life" series for its practical approach. Dr. Maria Fiatarone Singh, a prominent researcher in the field of exercise and aging, has long maintained that "the most dangerous thing an older person can do is nothing."
Health departments in the UK and Australia have begun integrating these findings into public health guidelines. A spokesperson for the British Geriatrics Society recently noted, "Moving from a model of reactive care to one of proactive strength-building is essential for the sustainability of our healthcare systems. Sarcopenia is not just a clinical diagnosis; it is a quality-of-life issue."
The consensus among stakeholders is that sarcopenia should be treated with the same clinical rigor as hypertension or osteoporosis. This involves routine screening in community health settings and the establishment of "strength clinics" where elderly patients can access specialized equipment and professional guidance.
Broader Impact and Implications for Public Policy
The shift toward viewing sarcopenia as a modifiable condition has profound implications for public policy and urban planning. If muscle strength is a prerequisite for independence, then society must provide the infrastructure to support it. This includes:
- Investment in Community Centers: Creating accessible spaces equipped for resistance training specifically designed for seniors.
- Physiotherapy Integration: Ensuring that Medicare and NHS-style systems cover supervised exercise programs as a standard treatment for those diagnosed with sarcopenia or pre-frailty.
- Public Awareness Campaigns: Educating the public that "taking it easy" in old age can be detrimental to health, and that lifting weights is a life-long necessity.
The "Strong for Life" series concludes that the management of sarcopenia is perhaps the most cost-effective way to reduce the burden on long-term care facilities. By preserving muscle function, we preserve the ability of the elderly to perform activities of daily living (ADLs), such as bathing, dressing, and walking independently.
Conclusion: Shifting the Paradigm from Frailty to Strength
The culmination of the "Strong for Life" series serves as a call to action for both clinicians and the aging population. Sarcopenia is no longer an invisible threat but a manageable condition with a clear path to recovery. Through the combination of early diagnostic screening, adequate protein intake, and, most importantly, supervised resistance training, the trajectory of aging can be fundamentally altered.
As the global population continues to age, the focus must shift from merely extending the lifespan to extending the "healthspan"—the period of life spent in good health. By addressing the "poverty of flesh" that is sarcopenia, medical science provides a blueprint for a future where aging is synonymous with strength and continued participation in the richness of life. The evidence is clear: it is never too late to start, and the benefits of becoming "Strong for Life" extend far beyond the muscle fibers themselves, touching every aspect of human health and societal well-being.